Incomplete tetraplegia is the most frequent neurologic category after spinal cord injury (SCI). Each year, nearly 12,000 people suffer from SCI in the United States, and about 50% of these are reported to be injuries at cervical lesions, representing mild to severe impairment in arm and hand functions. Over the years, life expectancy after injury has increased, which has resulted in increased economic burden to meet individual needs of hospitalization, home and vehicle modifications, medications, supplies and personal assistance.
Despite extensive pre-clinical and clinical research and advancements in rehabilitation strategies, there is still no “cure” identified for SCI and therefore, it continues to be a major cause of long-term disability. Given the fact that the majority of individuals with SCI are in their most productive years with a life expectancy nearly approaching those of the healthy population, more aggressive treatment strategies focusing on improvement of peripheral muscle control and functions, as well as the recovery of the central nervous system (CNS), are needed. More than half of the population with tetraplegia indicated that regaining arm and hand function would most improve their quality of life. Despite this evidence, a great deal of technology and research has focused on improving leg strength and retraining gait after SCI and not on upper-extremity strength and function. Furthermore, little research has been directed at understanding and optimizing interventions for the upper extremity when compared to gait training.
Neuroplasticity of the Central Nervous System
Since the work by Santiago Ramon y Cajal in 1928, the common assumption has been that the CNS is hardwired, which suggests that it is incapable of anatomical modification and self-repair. To some extent this assumption might have affected the approach of rehabilitation specialists in designing treatment protocols so that education of compensation techniques to regain independency in daily activities, such as using assistive devices to accomplish eating, dressing and transfers, has been emphasized over more aggressive treatment strategies. However, over the last three decades the view of the CNS has undergone fundamental change. Numerous studies from basic science provide evidence that the brain is capable of producing new nerve cells and that these neurons are interconnected with existing nerve cells. Even following injury or during the course of neurodegenerative diseases, the brain and spinal cord have the physiological ability to reorganize synaptic connections. Therefore, understanding brain and spinal cord plasticity will provide a basis for developing better treatment interventions to facilitate return of function after injury. In fact, evidence from animal studies was successfully translated into clinical practice of interventions to promote recovery of walking in humans. One example of this type of plasticity derives from basic science studies in which cats with complete spinal transections respond to intense walking training in the absence of supraspinal input.
Upper-limb Interventions after SCI
Studies of motor recovery of arm and hand functions after SCI are relatively limited and generally focused on functional electrical stimulation, exercise, neuroprosthesis, botulinum toxin injections, biofeedback or surgical interventions such as tendon transfers. In the last decade, introduction of robotic devices into rehabilitation has enabled semi-automated or automated high-intensity repetitive therapy, which otherwise would be quite labor-intensive (Takahashi et al., 2008; Kutner et al., 2010; Volpe et al., 2008). Intensity of treatment is an important determinant of recovery, and therefore, optimization of treatment protocols should focus not only on questions such as “context” and “when” but also on “how much.” Recent work in neuroscience demonstrates that treatment intensity has a profound effect on motor recovery and, even years after a neurological injury, neuroplasticity of the adult brain can be impacted by experience (activity)-dependent principles. Interestingly, studies have found that robotic-assisted therapy, in addition to traditional physical and/or occupational therapy, can improve motor recovery. Bringing robotics into rehabilitation provides additional advantages such as quantified assessment and monitoring of motor functions, bringing therapy to different venues including the home and increasing therapy efficiency with the possibility of group therapy. However, evidence-based randomized clinical trials are needed to promote recovery of upper-limb movements within the context of facilitating neural networks at the spinal and supraspinal level and thereby inducing intrinsic recovery mechanism and improving functions.
Preliminary Results
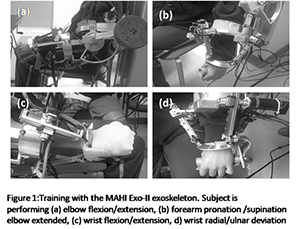
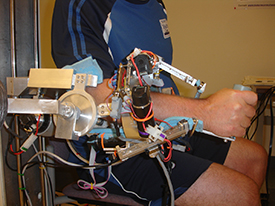
Over the past five years, our laboratory has been studying robotic-assisted combined treatment protocols in recovery of upper-limb motor functions after stroke and SCI. In a recently completed project, we used the MAHI Exo-II, from the Mechatronics and Haptic Interfaces (MAHI) Lab directed by Marcia O’Malley. PhD at Rice University, to study the feasibility, safety and efficacy of robotic-assisted training of arm and hand movements in persons with incomplete SCI. The subjects have completed 12 sessions of robotic training over a course of four weeks and were tested at baseline, after treatment and at six months for changes in motor functions and independence in daily living activities. Earlier work from this project was published as a case report in which a 28-year-old woman, 29 months after an incomplete SCI at the C2 level, classified as American Spinal Injury Impairment Scale C (AIS), received robotic-assisted training, based on her baseline motor abilities, either in constraint, triggered or passive modes (Yozbatiran et al., 2012). The positive gains in arm and hand movements suggested that highly repeatable active single-joint movements delivered through a rehabilitation robotic device can be safely implemented in treatment of upper-extremity training after cervical SCI.
To study the hypothesis of increasing excitability of the cortical motor region (M1) with anodal tDCS combined with robot-assisted arm training would provide greater improvement in contralateral arm and hand motor functions when compared to combined sham stimulation and robot-assisted training in patients with chronic, incomplete cervical SCI. A parallel-group, double-blinded, randomized, sham-controlled trial was designed. Eight participants with chronic, incomplete cervical SCI (AIS C and D level) were randomized to receive 10 sessions (5 daily sessions over 2 consecutive weeks) of anodal tDCS (2mA, 20 min; active group n = 4) or sham stimulation (2mA, 30s stimulation at the beginning and end of 20 minutes; control group n = 4) followed by robot-assisted training of upper-limb movements. Effects of tDCS were assessed with the Jebsen-Taylor Hand Function Test (JTHFT), and grip and pinch strength tests, at the beginning and end of treatment. In a subgroup of participants, corticospinal tract integrity was assessed using diffusion tensor imaging (DTI).
Conclusion
Given the strong evidence both from clinical practice and research, individuals with tetraplegia have a great desire to improve control of their arm and hand function. This evidence should lead rehabilitation researchers to combine their efforts with engineers and neuroscientists to design and develop treatment protocols with optimized frequency, intensity, duration and type of training.
References
- Yozbatiran, N., Berliner, J., O'Malley, M. K., Pehlivan, A. U., Kadivar, Z., Boake, C., & Francisco, G. E. (2012). Robotic training and clinical assessment of upper extremity movements after spinal cord injury: A single case report. Journal of Rehabilitation Medicine, Feb 44(2):186-188.
- Takahashi, C. D., Der-Yeghiaian L., Le, V., Motiwala, R. R., & Cramer, S. C. (2008). Robot-based hand motor therapy after stroke. Brain, Feb 131(Pt 2):425-437.
- Kutner, N. G., Zhang, R., Butler, A. J., Wolf, S. L., & Alberts, J. L. (2010). Quality-of-life change associated with robotic-assisted therapy to improve hand motor function in patients with subacute stroke: A randomized clinical trial. Physical Therapy, Apr 90(4):493-504.
- Volpe, B. T., Lynch, D., Rykman-Berland, A., Ferraro, M., Galgano, M., Hogan, N., & Krebs, H. I. (2008). Intensive sensorimotor arm training mediated by therapist or robot improves hemiparesis in patients with chronic stroke. Neurorehabilitation & Neural Repair, May-Jun 22(3):305-310.
- Kumru, H., Murillo, N., Samso, J. V., Valls-Sole, J., Edwards, D., Pelayo, R., Valero-Cabre, A., Tormos, J. M., & Pascual-Leone, A. (2010). Reduction of spasticity with repetitive transcranial magnetic stimulation in patients with spinal cord injury. Neurorehabilitation & Neural Repair, Jun 24(5):435-441.
- Roche, N., Lackmy, A., Achache, V., Bussel, B., & Katz R. (2011). Effects of anodal transcranial direct current stimulation over the leg motor area on lumbar spinal network excitability in healthy subjects. The Journal of Physiology, 589.11: 2813-2826.
Nuray Yozbatiran, PhD, PT, is an assistant professor in the department of Physical Medicine and Rehabilitation at McGovern Medical School. Her research interests include neurorehabilitation following stroke, spinal cord injury and traumatic brain injury; noninvasive brain stimulation with transcranial direct current stimulation and transcranial magnetic stimulation; neuroimaging with functional MRI; and diffusion tensor imaging.
Subscribe to the TIRR Memorial Hermann Journal
Nationally Ranked Rehabilitation
For the 35th consecutive year, TIRR Memorial Hermann is recognized as the best rehabilitation hospital in Texas and No. 2 in the nation according to U.S. News and World Report's "Best Rehabilitation Hospitals" in America.
Learn More